Patients with bilateral posterior crossbites tend to have deep palates and bilaterally extended cervical chains. Depending on the degree of interdigitation of the teeth, the balancing interferences of the lingual cusps of the lower molars against the buccal cusps of the upper molars can make the canines out of position from a functional standpoint.

Consultation with an oral surgeon may lead one to believe that a two-jaw surgery plus braces is the only way to correct the defect. But the dysfunction that is created by this seemingly backward bite rarely happens during function, and happens instead during parafunction; in other words, surgical correction may not be necessary if function can be addressed properly.
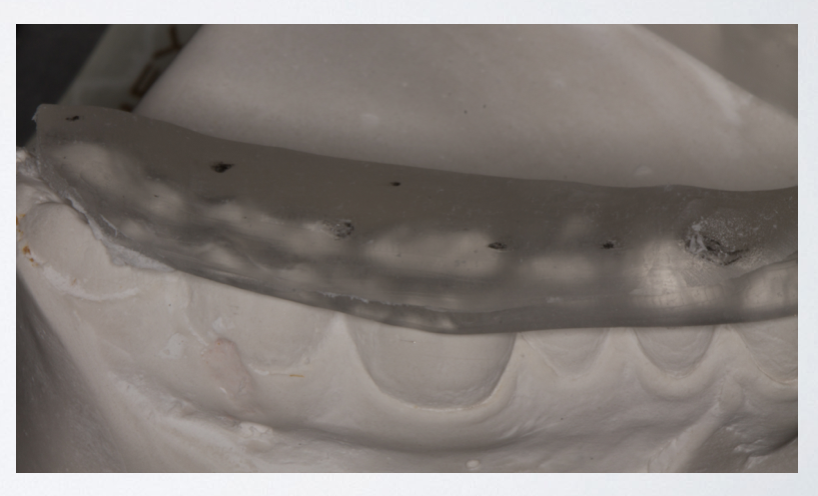
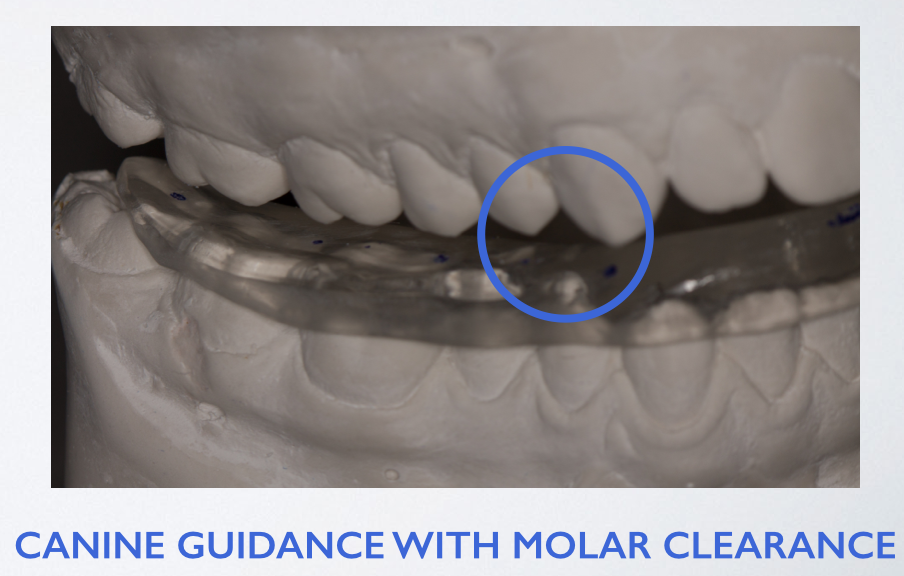
A lower bite splint can be designed to create the sensation the canine has needed for cervical-axial rotation, by giving more immediate lift to the canine, and creating more freedom in the posterior section by creating a smooth transition. While it is frequently difficult to engage the upper lingual cusp of the molar on the splint without having the tooth slide across the splint, it is preferable to have that cusp engage and gently and smoothly slide across (rather than using the upper buccal cusp to maintain the posterior contact and have no lateral occlusion on the splint). However, in the transitional zone where the normal anterior bite crosses the bite to become an inside-out posterior bite, the buccal cusp tip of the premolar can be used for light contact and light excursion stroke.